Team members: Debargha Dey, Ruud Zandbergen, Victor Donker
Advisor: Jacques Terken, TU/e
Role: User researcher
ABSTRACT
A neonatal intensive-care unit (NICU), also known as an intensive care nursery (ICN), is a unit of a hospital specializing in the care of ill or premature newborn infants. This is a high-pressure, high-intensity environment which requires the nurses to stay alert and respond immediately to alarms which can be indications of an infant requiring a life-saving intervention. It is imperative that in this environment, the nurses are able to direct their full attention to the infants under care, and hence, the interfaces of the system that they use in their work should be as intuitive and seamlessly integrated into their workflow as possible. I did a study with my team to investigate some aspects of the NICU interaction process that currently inhibit nurses in functioning to their fullest potential and an exploration of potential solutions.

NICU incubator
OBSERVATIONS
In an attempt to find context for the problem and identify the process of a Neo-natal Intensive Care Unit (here onward abbreviated as NICU), we visited the hospital MMC (Máxima Medisch Centrum) Veldhoven and were given a guided tour of their NICU by Astrid Osagiator, a Senior Nurse in their Neonatalogy department. Our takeaways from this experience are summarized below.
NICU is a place where premature infants are given intensive care so that they are able to transition into high-care units (where they will need further monitoring and care before they van transition into the outside world). Since premature infants are sensitive to stimuli, the lights in the rooms are dimmed, and a cover is placed in the incubator so as not to disturb the infant. Care is triaged and prioritized, so even at full capacity, each nurse has at most 3 infants to monitor. The infant’s vital signs are displayed on a screen/ monitor attached to the incubator. However, a nurse can bring up the vitals of another infant in another room as a pop-up window on the monitor of the room.
Each nurse carries a phone/ paging device which alerts them in case of an alarm with an infant under their care. The alerting system filters and sends only critical alarms to the nurses’ pager. Once an alarm is received, the nurse must respond to it by pressing a “confirm” button on their pager the alarm for it to stop ringing. If the alarm is not confirmed in 10 seconds, it is forwarded to a backup nurse (at which point the alarm for the primary nurse stops ringing). If the backup nurse also fails to respond to the alarm in 10 seconds of receiving it, the alarm is sent to all devices of all the nurses in the unit. The alarms also sound at the monitor in the infant’s room, but at minimal volume.
PROBLEM IDENTIFICATION
Based on our observations, and following a conversation with Astrid, we identified some core areas in which interaction methodologies cause some frustration for the nurses. These are summarized below:
- Sometimes when multiple alarms arrive in a close succession at the nurses’ pager, it can be overwhelming for them.
- When an alarm arrives from another room, the nurse has to actively “confirm” a message on their pager, and manually pull up the vital stats of the infant for whom the alarm was triggered. This can be time consuming and cumbersome, especially if they are working on something else and their hands are occupied.
- To see details about the alarm and gain insights on the vital statistics or trends of the infant, the nurses have to manually bring up the details of another room from where the alarm was generated. This usually appears as a small pop-up window on the same monitor.
- Most of the alarms occur when the nurses are actively working on the infant. When the sensors are disturbed or detached, it often triggers an alarm. This is annoying for the nurses because they are right with the infant at that point, and don’t need an alarm for what they are clearly aware of. They are able to disable alarms from the monitors for a short period of time when they work with the infant, but it doesn’t synchronize with their pagers, and they still get the alarms on their mobile devices.
- There are currently no means by which the nurse can see the infant from another room (e.g. a live video feed). This would help a nurse in analyzing the urgency of a situation when an alarm goes off.

NICU monitoring display
PROBLEM SELECTION
Based on the multifaceted and dependent nature of the problems identified, we decided to address them piecemeal, and share the task with other groups. Since a large number of problems identified revolved around the context awareness of the system (whereabouts and current activity of the nurses: problems 2, 3, and 4), we decided to focus on the problem that the nurses don’t have immediate and comprehensive knowledge of the state of other rooms (problem 5).
Given that context awareness can be solved and implemented, it will also help in the better implementation and integration of our proposed solutions into the system.
We focus on the problem that when an alarm goes off for a nurse who is already occupied in working with another infant, there is no way for the nurse to immediately check on the details of the infant for whom the alarm was triggered. A context aware system will know which nurse has which nurse is assigned which infant, as well as which nurse is in which room. Based on this, we will be looking at ways the information from other rooms can be brought to the nurses with minimum input from them (as opposed to them manually pulling up the information of another room). This will help the nurses gauge the urgency of the situation and help them prioritize and triage their attention.
DESIGN STATEMENT
We intend to propose a solution in which all relevant information about an alarm-generating infant can be delivered/ displayed to the nurses at the right time with minimal intervention and without compromising the privacy of the parents in the room.
There are 3 distinct questions that arise from this statement:
- Right time/ minimal intervention: Currently, the nurses need to manually pull up a screen containing details from another room if they need this information. A context-aware system will be able to identify which nurse is in the room, and which infant’s information she needs to see. Based on this, she may be provided with options of when she would like to be presented with this information.
- How/ where this information is presented: Currently, when the nurses pull up the information about another room, it appears as a small pop-up display on the current screen, which is difficult to read. We need to explore what alternatives, if any, can provide a realistic, easy, and cost-effective way of presenting this information may be recommended.
- Relevant information: We ask what consist of relevant information; what the nurses need to see, and how much is too much information.
It can be noted that these questions can be summarized under 3 headings:
- When to display
- How/ where to display
- What to display
An overarching theme in this entire solution is the issue of privacy. We needed to be mindful that no solution can compromise the sense of security the parents share in the NICU, which is an integral component of this care.
IDEATION
We conducted a brainstorming session to generate ideas that match with our design statement in 3 categories.
When to display
This focused on the moment and action that cued the presentation of information about other infants. We came up with a number of possible ways of accomplishing this such as:
- Speech recognition – the nurse can speak a keyword to the system which recognizes it and turns on the information feed
- Eye-tracking – sensors can detect if the nurse in the room has acknowledged the alarm, and bring up the information feed
- Automatic control – an intelligent, context-aware system can identify which nurse is in the room, and immediately bring up the relevant information about the infant in distress without any input from her whatsoever.
How/ Where to display
We realized that the one monitor that the nurses currently use is already crowded with information, and any additional information on a smaller display will add to the cognitive load of the nurses. We understood the need for a different mediums to display information, came up with a few alternatives regarding the display medium and place, such as:
- A simple additional screen to the already existing monitor which normally stays off, but turns on to show alarm information when there is an emergency.
- Projection on the incubator, wall, or floor – this would be another inexpensive way to show extra information, although there may be need for considerations for readability and privacy,
- Smartwatch – alarm goes the smartwatch and can be confirmed using gestures (or touch)
- Hologram interface – provides information about the alarm and the distressed infant. This can provide the vital statistics of the infant, as well as the patch sensor location, including which sensor(s) generated the alarm. Another alternative may be to have a 3D infant projected in the hologram.
- Leap motion – manual gestures can be used to control screens outside the incubator when the nurses have their hands inside the incubator.
- Physically sliding screens – that emerge from behind the primary monitor of the room, and go away when there is no emergency.
- Headset/earpiece – with information provided directly to nurses (eliminates privacy concern).
- Consideration – An intermediate nurse who judges the importance of an alarm and directs them to correct nurses.
What to display
Here, we focused on ideas that revolved around what kind of information could be presented to the nurses to know what is happening with an infant in another room.
The simplest idea was that of a live video feed of the infant which can be displayed to a nurse in a different room. However, this could be interpreted as intrusive, and depending on how the camera is placed in the room/incubator, it can show more of the room than the infant, which isn’t desirable. Alternatively, as seeing the infant itself might not be a necessity, we thought of the possibility of showing a static model outline of an infant that gives the nurses information about certain vital statistics. An improvement over this would be the combination of both these ideas, which involves using image processing techniques to show the outline of an infant, accompanied by only the relevant features to the nurses. Each of these systems would work to provide continuous feedback when it is on.
While “when”, “how”, and “where” were valid questions for the purpose of this study, for our work we decided to focus on the “what” question. Since some of the former questions were being addressed by other people at the time of this study, we decided to accept some of the less technically and financially constrained alternatives of these questions. Taking realistic feasibility into account, we assumed that a plausible medium of displaying this information will be a secondary screen, or a smartwatch (as opposed to a holographic projector, for instance). We also assumed that a context-aware system can address the automatic displaying of this information. Such a system will be able to monitor when the information will have to be provided to the nurses, so we refrained from focusing on this aspect further.
DESIGN ALTERNATIVES
The ideas were re-assessed and led to four design alternatives that will be discussed in more detail below. Each of these information will be shown in addition to the vital statistic and trend data that the nurses are already able to see, so as to give more context information to the nurses and augment their situation awareness.
Static model infant
This is a simplistic solution that shows an outline of the infant on the monitor, along with a representation of the spatial orientation of the sensor patches. Normally, the sensor patches in this display will be white, which would indicate that everything is stable. In the case of an alarm, the representation of the sensor patch that triggered the alarm will change color to red, and may even flash. Additional information for that sensor will then also be shown on screen. The sensor patches on the model infant may not be compliant with the location of the patches on the actual infant, as there is no standard way of placing the sensor patches.
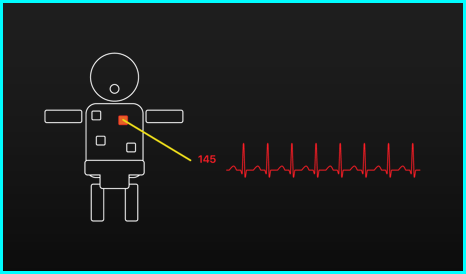
Static model infant display
Static model infant (extra animated)
As the static model infant is a very simple representation of the infant, it is not able to give information about the actions or reactions of the infant. An extended version of the static model infant may be able to show this information by using simple icons. This means that this design alternative is very much the same as the first alternative, but with added functionality to provide extra information, such as when the baby is moving, or crying.
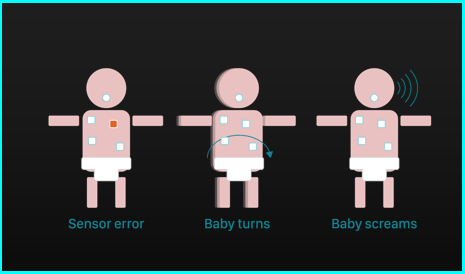
Extra-animated static model infant display
Live video feed of infant
One of the most important pieces of information that the static model infant cannot provide at this point is information about what the infant is exactly doing and about the position of the infant. The position of the infant can give extra information about what may have happened to cause a certain alarm. Sometimes this will accelerate the treatment due to a better sense of the situation, and in other cases, it will, for example, show a loose sensor patch that is causing a false alarm. A live video feed showing the incubator could provide more information such as the aforementioned position of the infant. The video feed does raise questions about possible privacy issues for the infant and the parents. The video feed also asks for a lot of cognitively loaded processing from the nurses, as they will need to do a lot of observing and interpreting to get a good understanding of the situation.
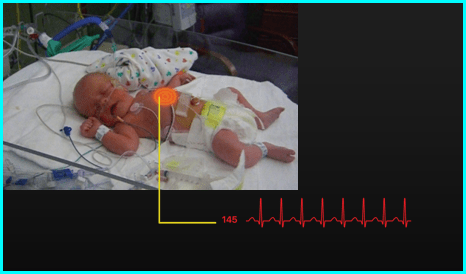
Live feed display of infant with sensor highlight
Image processed video feed of the infant
The last design alternative combined the ideas of the model infant and the video feed. By using image processing software we would be able to make a video of the infant and create a new output that only shows the relevant features of the infant, and remove all unnecessary background information. As is visible in the figure above, this alternative would consist of the outline of an infant with the sensor patches made clearer. This alternative would be able to show the position of the infant, a clear overview of where the sensor patches are and can give additional information on screen too. As only an outline is shown, this is less prone to privacy issues than the live video feed. However, there are still some doubts about how realistic this method is with regard to the technology. The calculations that have to be done to process the images frame by frame are very costly, so it may be possible that there will be delays in the images that nurses receive. Since every second counts in a safety environment such as the NICU, it may be undesirable to have a (large) delay in the images you are receiving. Secondly, such a system would probably also be very expensive.
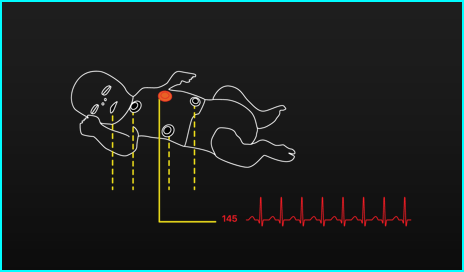
Image-processed display of infant filtering only “need-to-know” information
COGNITIVE PRINCIPLES
A number of cognitive principles were used when designing the four discussed alternatives. These principles will be discussed one by one below.
Pictorial realism: the model/outline of the infant can be seen as a use of pictorial realism. It represents the infant with an image that is very close to the real situation.
Visual contrast and color coding: The model infant and the image processed infant both included a black background with a white outline. This was done to make sure that an optimal contrast was achieved. The other elements on the screen were depicted using colors, but we tried to minimize our use of different colors to make sure that it was easy to distinguish between the different elements.
Visual clustering of information: We attempted to make sure that all the relevant information would be presented in one place. We did not decide on how to present the information yet, because we were working mostly with assumptions for this point. We envisioned that our design alternatives would be displayed on the current monitor, or on a secondary monitor directly beside the current monitor. This way we would reduce the need for scanning for the nurses as all relevant information would be clustered. We also tried to prevent visual clutter by only presenting useful information as much as possible, especially in the model infant and the image processed infant.
Consistency of sensor placement and mapping: The concept of mapping was used to show that the sensors in the model would comply with the sensors on the infant. This was not completely possible for the static model infant, since the sensors are not always placed at exactly the same location on every infant, but it is impossible for the sensors to tell where they are placed on the infant. We have to be aware of the possibility that an unclear mapping on the static model infant could lead to errors, so this should be investigated further.
Information processing: There are different levels of cognitive processing necessary for our different design alternatives. The static model infant is a very simple concept, so this can give information very quickly without much effort for the nurse. However, this concept cannot show as much information as the other alternatives. The video feed has the highest cognitive load, as this has to be completely interpreted by the nurse. The exact impact of the cognitive load for the four alternatives have to be evaluated further before we are able to draw any conclusions about this.
FUTURE WORK
We made a number of assumptions about the thoughts and preferences of the nurses and parents, so it would be valuable to get their actual input on some subjects. We also had a few ideas that we did not incorporate in the design alternatives at this point due to time issues or because we thought this had to be investigated first. One of these things would be to use the concept of redundancy gain for the sensor information in our alternatives. They were white in a stable state and red in an alarm state at this moment, but it could be interesting to see if it is possible to match their colors to the colors on the current monitor in the NICU room. It is very important to see if this does not lead to more errors due to wrong interpretations of the colors but it could help to map the sensors better.
We also thought about the possibility of using multiple resources to display information. The visual input that we have chosen so far could be supplemented with auditory input. By using auditory input the issue of privacy that is potentially present could be addressed, as a nurse could be the only one to receive the input in an earpiece. Here, it is important to see if the use of multiple resources does not negatively influence the attention of the nurses.
CONCLUSION
We created four design alternatives that may be able to support nurses in their work in the NICU. The designs will be able to help nurses with understanding what is happening to infants in other rooms than they are present at that particular time. The principles of cognitive psychology were used during the creation of the design alternatives, but some of these principles were applied using assumptions. The cognitive principles showed us a more theory-grounded way of designing that helps to make design decisions based on proven concepts. The use of these concepts will not only be very valuable for this NICU case, but for designing in general.
Disclaimer: Full article available on request
